Diagnostic dilemma: A parasite never before seen in humans was behind a woman’s lung infection, organ damage and forgetfulness

The patient: A 64-year-old woman in New South Wales, Australia
The symptoms: The woman was admitted to hospital after suffering from abdominal pain and diarrhea for three weeks. She also had a persistent dry cough and night sweats.
What happened next: Three weeks later, the woman returned to the hospital with a cough and fever, although she was still taking prednisolone, and the lesions on her organs had not healed.
Further tests failed to identify the cause of his respiratory distress. Cultures of tissue samples showed no signs of bacterial or fungal infection. Blood tests showed that his immune system did not produce antibodies against various parasitic flatworms, such as blood flukes (Schistosome) or liver flukes (fasciola). There was also no evidence of the presence of these parasites in his fecal samples.
Doctors advised the patient to continue taking prednisolone and also prescribed ivermectin, a treatment for parasitic worms, because she had informed doctors that she had traveled to countries where these parasites are common.
But her respiratory symptoms did not go away and they worsened when she tried to reduce the dose of prednisolone. His condition remained unchanged for several months.
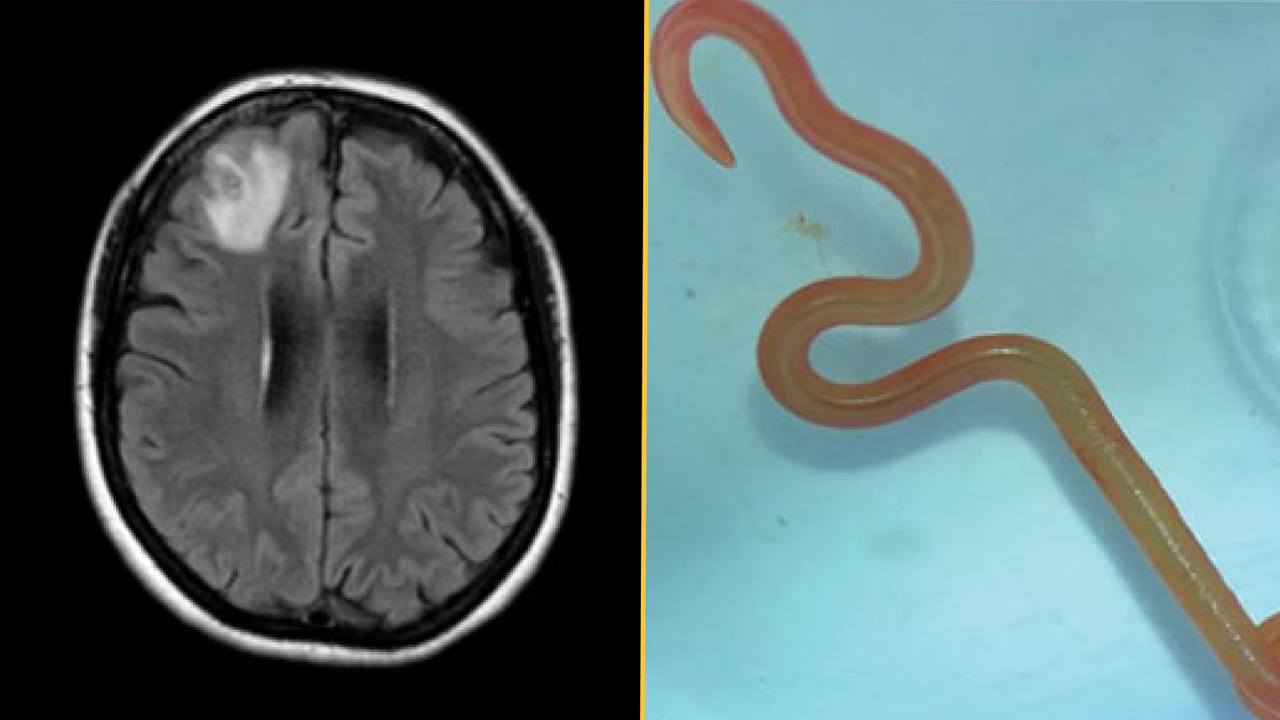
The diagnosis: About a year after her first hospital visit, the woman began to develop signs of depression and have episodes of forgetfulness. Doctors ordered an MRI of his brain and detected a lesion on his right frontal lobe. They then performed an open biopsy to expose and examine the damaged area. That’s when they discovered “a thread-like structure” inside the lesion, which they identified as a live parasitic worm called a helminth, according to a report of his case.
The worm was bright red and measured about 3 inches (80 millimeters) long and 0.04 inches (1 millimeter) thick.
The treatment: Doctors removed the helminths from the woman’s frontal lobe and examined the surrounding tissue, where they no longer found parasites. They gave him ivermectin for two days, this time in combination with a four-week course of albendazole, a broad-spectrum drug for treating helminth infections, to kill any lingering parasites in his organs.
Albendazole is absorbed by the central nervous system more quickly than ivermectin, and these drugs have previously been used together to treat nematode infections in humans and snakes. The patient also received a 10-week course of dexamethasone, a corticosteroid, to prevent further inflammation.
Six months after the operation and three months after the end of dexamethasone treatment, the lesions in the patient’s lungs and liver had disappeared, her white blood cell count was normal, and her neuropsychiatric symptoms had improved.
What makes the case unique: Doctors identified the helminth as a third instar larva of Ophidascaris robertsia type of parasitic nematode native to Australia. Adult worms breed inside carpet pythons (Morelia spilota), but the nematode can infect other animals during the larval stages of its life cycle.
Carpet pythons were common near the woman’s lakeside home, and although she didn’t remember having direct contact with snakes, she often fed on wild greens for cooking. She likely became infected after touching or eating plants contaminated with O. robertsi eggs, the authors of the case report suggested. After the eggs hatched, the larvae migrated to its organs.
The longevity of this larval infection was not unusual, since laboratory rats can harbor O. robertsi larvae for more than four years, according to the report. However, no human infection with this parasite has ever been documented, and the parasite larva has never been found in the brain of its host.
For more intriguing medical cases, check out our Diagnostic Dilemma Archives.
This article is for informational purposes only and is not intended to offer medical advice.
Hossain, M., Kennedy, KJ, Wilson, HL, Spratt, D., Koehler, A., Gasser, RB… Senanayake, SN (2023). Human neural larva Migrans caused by Ophidascaris robertsi Ascarid. Emerging infectious diseases29(9), 1900-1903. https://doi.org/10.3201/eid2909.230351



