RSV is surging, but antibody shots and vaccines can protect babies

January 20, 2026
4 min reading
 Add us on GoogleAdd SciAm
Add us on GoogleAdd SciAm
RSV is on the rise: Antibody shots and vaccines can protect babies
Respiratory syncytial virus cases are increasing, but vaccines and antibody shots can keep young children out of the hospital

Nirsevimab (Beyfortus) is one of two RSV vaccines available in the United States.
FRED TANNEAU/AFP via Getty Images
Winter illnesses hit the United States. A mutated flu variant is sending dozens of people to hospitals, 32 children have died from the flu so far this season, whooping cough has killed more than a dozen people, and now respiratory syncytial virus (RSV) is on the rise.
In the United States, RSV season typically peaks in January and February, with cases often extending into March. Nationwide emergency room visits and hospitalizations due to the virus among children ages four and younger have declined slightly but are increasing overall in more than a dozen states, according to the latest report from the Centers for Disease Control and Prevention on Jan. 16. Overall RSV activity is increasing in many regions; national wastewater monitoring sites, which can predict future waves of infection in communities, have detected the virus in high concentrations.
“RSV is a very big problem, but we have very effective interventions,” says Yvonne Maldonado, a pediatrician at Stanford University School of Medicine.
On supporting science journalism
If you enjoy this article, please consider supporting our award-winning journalism by subscription. By purchasing a subscription, you are helping to ensure the future of impactful stories about the discoveries and ideas shaping our world today.
New studies showing that RSV vaccination during pregnancy and doses of protective antibodies given to babies in the first eight months of life are both highly effective in preventing serious illness in infants. This protection can even last beyond one RSV season. But the CDC currently reports suboptimal RSV vaccine coverage for children and adults — and experts fear those rates will continue to suffer given recent overall reductions in vaccine recommendations for children. Additionally, unfounded doubts about RSV vaccination, fueled by Health and Human Services Secretary Robert F. Kennedy, Jr., could pave the way for a more dangerous RSV season.
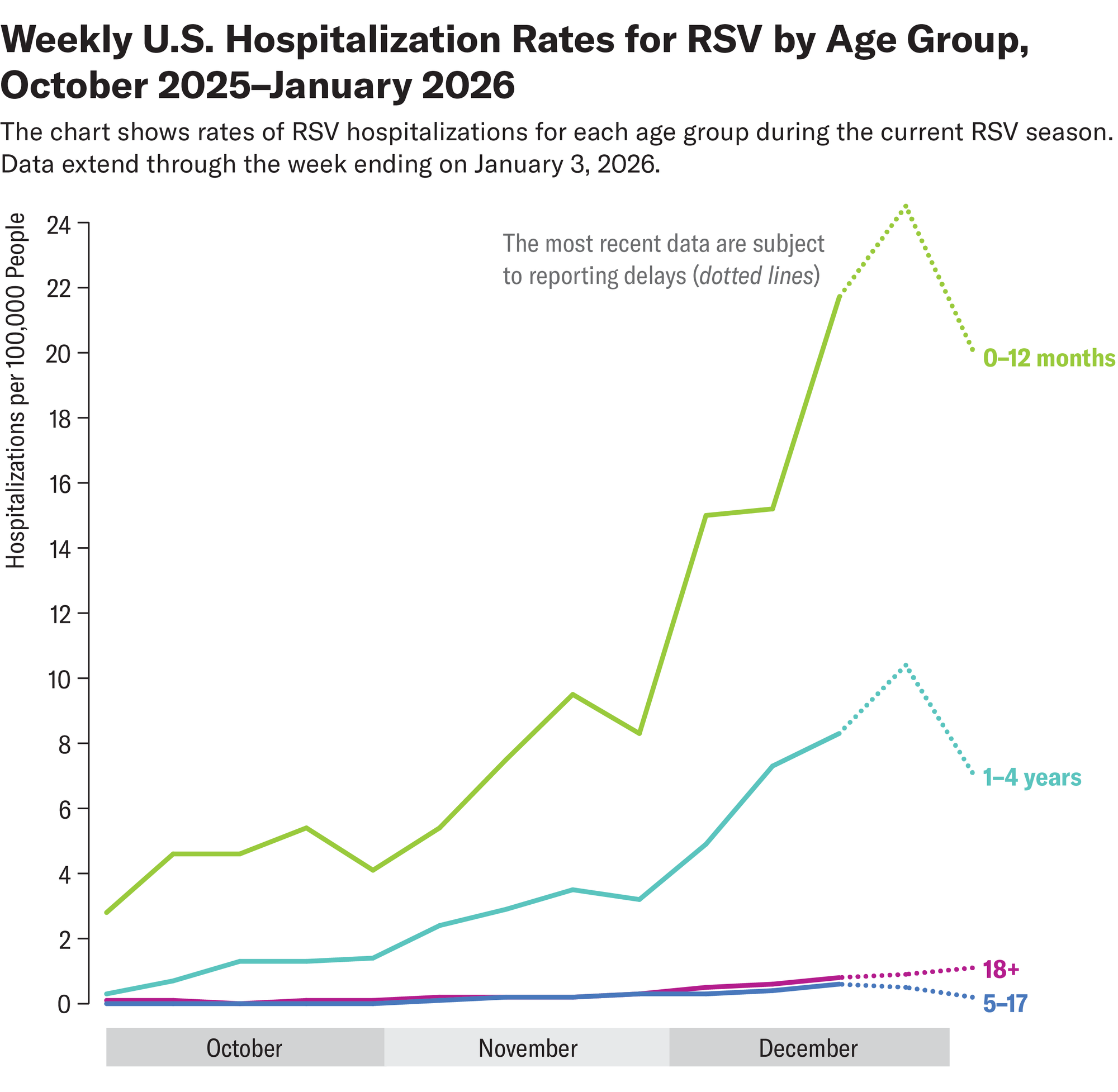
Almost everyone is infected with RSV at some point in their life. For most healthy individuals, it causes a severe cough, runny nose, or fever. The virus can also cause serious illness and long-term complications in older people. And infections can be especially life-threatening for young children: The virus is the leading cause of infant hospitalization in the United States, with the highest risk in the first two months of life. In babies, RSV can cause serious lung infection or pneumonia and, in extreme cases, death.
“RSV is a virus that causes the body to secrete a lot of mucus that can get trapped in the tiny airways of little babies and cause many breathing problems,” says Ruth Karron, a pediatrician and director of the Johns Hopkins Vaccine Initiative. “Children who are otherwise healthy may need respiratory assistance. This is a very serious illness.”
Fortunately, in 2023, two very effective tools became available in the United States to protect newborns, whose immune systems are not fully developed, from RSV during the first months of life. The vaccine for pregnant women, which is recommended during the RSV season to be administered between 32 and 36 weeks of gestation, strengthens antibodies against the virus that are transferred to the fetus via the placenta. These antibodies target a surface protein of the virus, preventing it from binding to human cells.
If a pregnant person does not receive the vaccine or is not eligible during RSV season, babies can receive protective antibodies directly through monoclonal antibody injections during the first months of life. These injections are not vaccines. A dose of one of two available monoclonal injections, nirsevimab (Beyfortus) or clesrovimab (Enflonsia), is recommended for infants eight months and younger and should be given just before RSV season to ensure protection lasts during the months when the virus is most active. A second dose may be given to older and higher-risk children, such as those born prematurely.
“Babies who receive the vaccine or monoclonal antibody can be protected against RSV for six months or more,” says Maldonado.
Both options are very effective and safe, but recent studies suggest that monoclonal antibodies may have additional benefits over vaccination.
A recent large study from France found that the nirsevimab antibody injection was associated with a lower risk of hospitalization and serious complications from RSV than the vaccine administered in utero. This difference became more apparent during subsequent follow-ups, beyond the first month of life, explains pharmacoepidemiologist Marie Joelle Jabagi, lead author of the study. “This suggests that the duration and timing of protection may play an important role in actual effectiveness, particularly over a full RSV season,” she says.
One explanation for these results could be that nirsevimab confers direct and immediate immunity to the infant and relatively uniform antibody levels. On the other hand, protection against the vaccine depends on the timing of vaccination and the effectiveness of the transfer of antibodies across the placenta, explains Jabagi.
Another study published last week found that nirsevimab reduced first-time RSV hospitalizations among infants in Spain by 86% during the 2023-2024 season. The data also suggests that some babies’ protection even lasted into the following season.
Experts emphasize, however, that even if these recent studies show that nirsevimab can offer greater and longer-lasting protection, the vaccine intended for pregnant women remains a very effective tool for preventing severe forms of RSV. “I think all of these products are phenomenal,” says Karron. “If used appropriately, they could really have a huge impact on RSV-related hospitalizations.” »
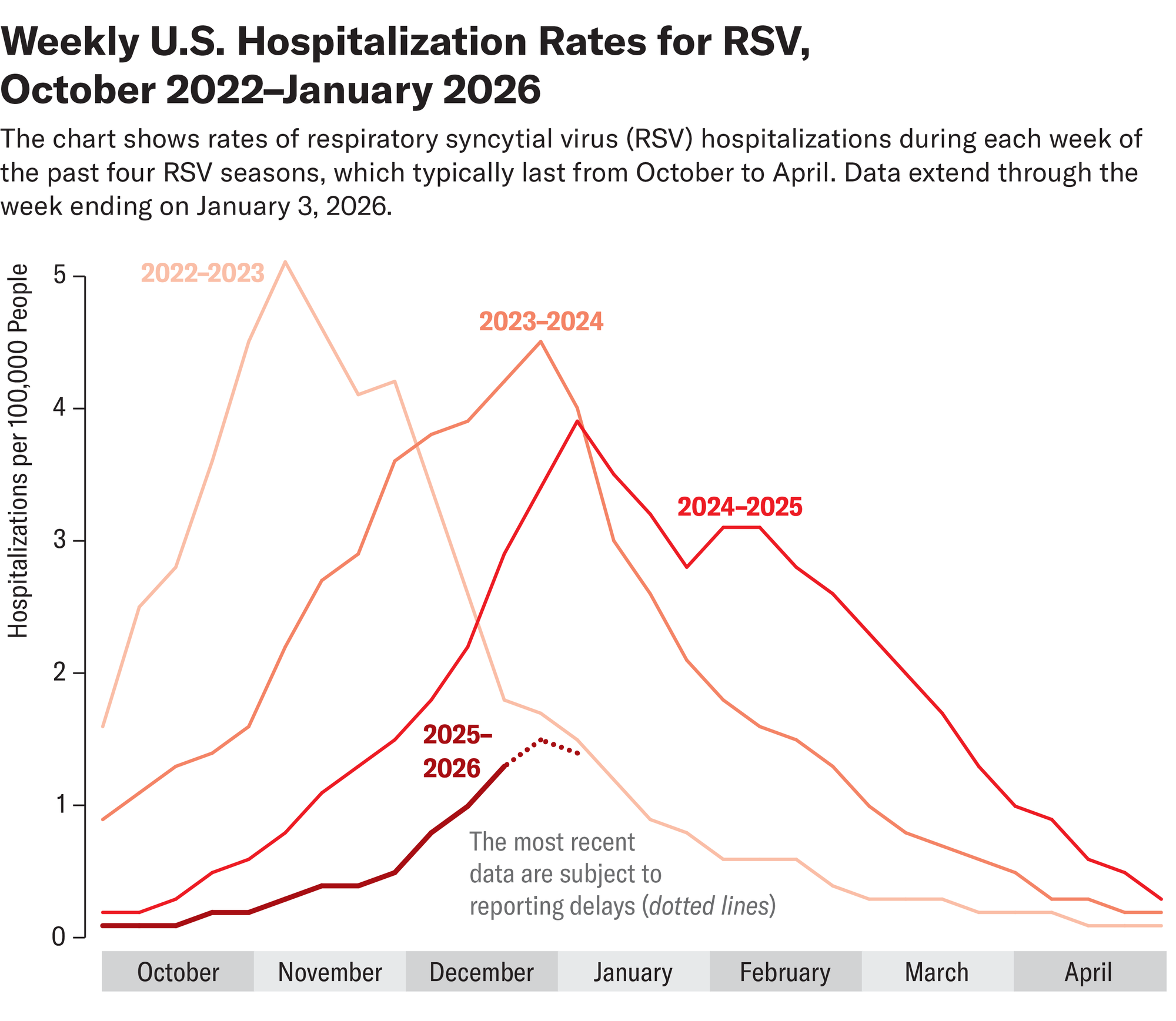
This impact is already being felt in the United States: during the 2024-2025 season – the first season after the vaccine and nirsevimab became available – RSV hospitalization rates fell by up to 43% among children aged zero to seven months. But experts fear that momentum is fading due to the Trump administration’s recent overhaul of the childhood vaccination schedule. Recommendations for maternal RSV vaccine and monoclonal antibody doses remain technically unchanged but place greater emphasis on high-risk infants. Karron worries the language could confuse some parents.
“If you have a healthy, full-term baby, you don’t consider that baby a high-risk child. If you read this and it says ‘high-risk children only,’ that’s an incredible deterrent,” she says. “We really hope that these products continue to be used so that we can keep children healthy. »
It’s time to defend science
If you enjoyed this article, I would like to ask for your support. Scientific American has been defending science and industry for 180 years, and we are currently experiencing perhaps the most critical moment in these two centuries of history.
I was a Scientific American subscriber since the age of 12, and it helped shape the way I see the world. SciAm always educates and delights me, and inspires a sense of respect for our vast and beautiful universe. I hope this is the case for you too.
If you subscribe to Scientific Americanyou help ensure our coverage centers on meaningful research and discoveries; that we have the resources to account for decisions that threaten laboratories across the United States; and that we support budding and working scientists at a time when the value of science itself too often goes unrecognized.
In exchange, you receive essential information, captivating podcasts, brilliant infographics, newsletters not to be missed, unmissable videos, stimulating games and the best writings and reports from the scientific world. You can even offer a subscription to someone.
There has never been a more important time for us to stand up and show why science matters. I hope you will support us in this mission.



:max_bytes(150000):strip_icc()/Health-GettyImages-SideEffectsOfNotWearingSunscreen-b3d208ce72504c17872e9e94780f3a90.jpg?w=390&resize=390,220&ssl=1 "8 Serious Side Effects and Risks of Not Wearing Sunscreen Every Day")
